3 Financial Truths All Medical Residents Will Be Shocked To Know

Medical residency programs are notoriously known for their rigorous and relentless training, and understandably so as you are preparing residents to become the physicians of the future, and taking care of people is one of the hardest things to do, with long-lasting effects of every decision a physician make on the life of his/her patients.
I remember working as a resident not too long ago for seemingly endless hours, ranging from those sweet, yet so rare, 60-hour weeks when you are on some outpatient rotations, to the monstrous 80–90 hours a week in medical and cardiac intensive care units, with 24–28 hour stretches of no sleep and constant work.
At the time, I didn't have a clear grasp of financial incentives and proper compensation. All I cared about is studying, rounding, performing procedures, and presenting lectures with the sporadic required research work that we had to do. Now, as an attending, I feel we, as physicians, do not really know much about how severely underpaid our residents are, trapping them in an illusion of training for a higher purpose, preventing them from asking for their rightfully deserved pay.
Once I started my job as an attending physician, I took it upon myself to educate myself about all the things I need to know to get a grasp of the financial aspects of our life as physicians that we so often neglect. Deep dive after another, made me reach those hard truths about medical residency training, that I want to share with you.
1 . Residents are overall severely underpaid
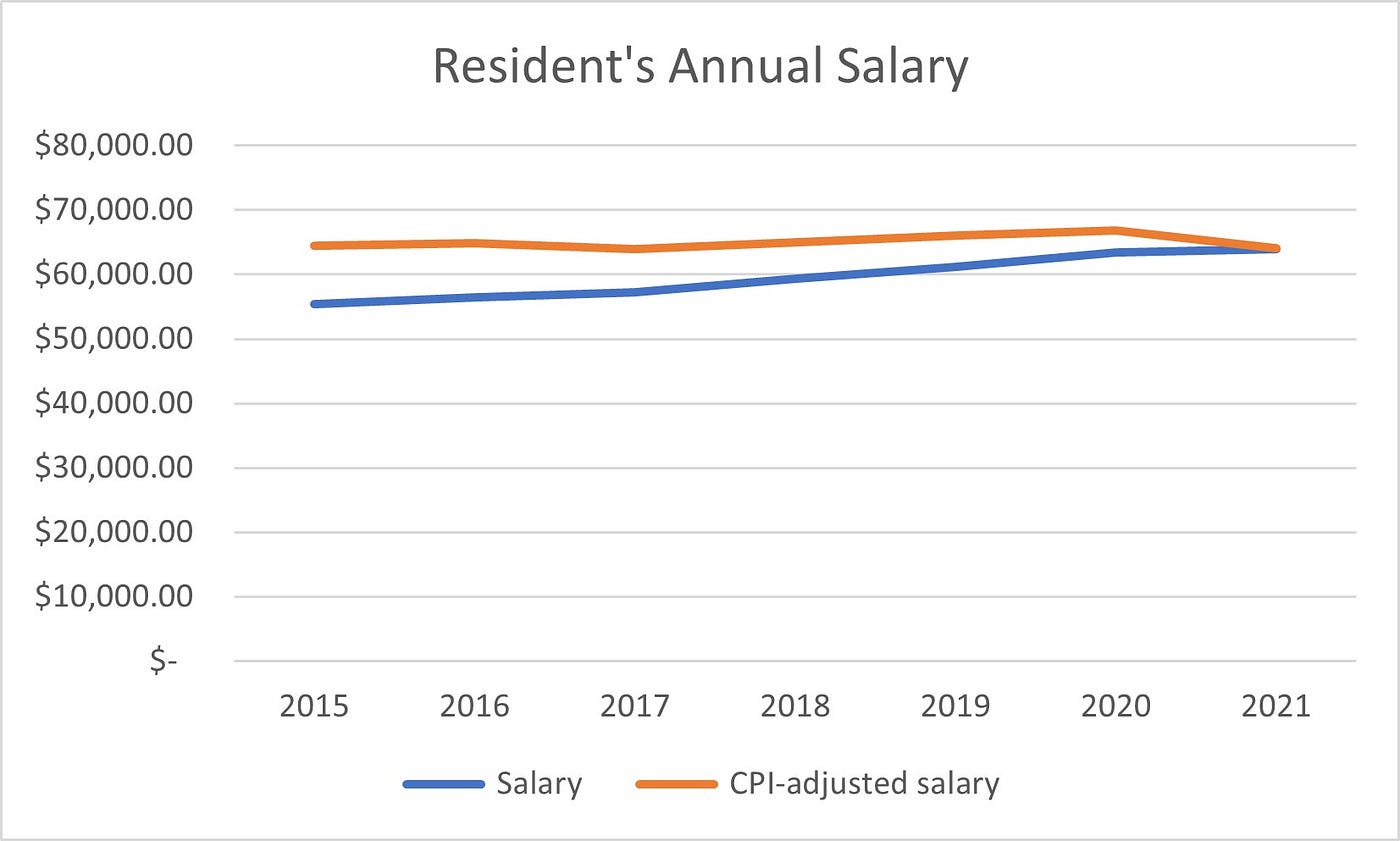
Data collected from Medscape regarding medical residents' compensation is used to generate this chart, this includes the average annual resident salary, with multiple factors that affect resident salary including location, year of training, and specialty of training.
For the layman, this seems like a gradual and appropriate increase In salary over the last 7 years, but on a deeper level, once adjusted for the Consumer-Price Index (which is a measure of inflation), we notice that residents' compensation has been stagnant over the years, with ~$55,000 in 2015 (~64,000, adjusted for inflation), to $64,000 in 2021.

One of the major reasons for this is the illusion sold to residents that this is only training years and you will be compensated properly once graduated, another more obscure reason, is the lack of ability of residents to negotiate their contracts, a topic I covered extensively in my previous post.
2. Residents work long hours with no compensation adjustment

As detailed above, the more hours a resident works, the less hourly pay he receives, as their annual salary is fixed and there is no structure for overtime compensation.
ACGME, a body that regulates graduate medical education, capped the maximum amount of hours a resident can work at 80 hours per week and does a fairly good job at enforcing it, but still, with the 80-hour week assumption, average hourly pay of $15.63/hour is abysmal.
That, of course, does not include the hours that residents fail to document or choose not to report fearing certain repercussions from their programs. According to the latest Medscape survey, 22% of residents spend more than 70 hours/week in the hospital taking care of patients, while it is a comprehensive survey, one thing that was not mentioned is how many hours do residents take their work home to finish up on all the piled up paperwork.
3. Hospitals benefit financially from having a residency program
Residents are funded by 2 mechanisms created by Medicare; direct and indirect Graduate Medical Education (GME) payments. Direct GME payments from medicare cover residents’ salaries, salaries of supervising faculty, and administrative costs. Indirect GME payments cover the cost to support unique features of teaching hospitals such as burn or trauma units or treatment of complex patients, along with the additional time it takes for patient care conducted by learners (residents).
It is estimated that training a resident costs around $150,000/year, most of which is covered by direct and indirect GME payments, the rest can be made up from Medicaid and Veteran Administration funding. Expenses beyond that are paid by the hospitals with residency training.
Research into the cost-effectiveness of resident training is conflicting and extremely complicated owning to the structure of compensation by both direct and indirect means. The most illuminating piece of data analysis comes from RAND corp research, with a detailed analysis of the current payment structure and impact on productivity and compensation; The benefits of hiring a nonphysician practitioner do not seem to outweigh that of training a resident, except in some subspecialties.
Final thoughts
We have an ethical obligation to educate our residents about financial literacy and enable them to make decisions based on knowledge and understanding of the current reimbursement model.
Better compensation models need to be put in place, to make sure that our hardworking residents get the pay they deserve and get compensated for the extra hours they put in along with shifting the current paradigm of thinking to a more financially sound one.
Twitter: https://twitter.com/AngryDoc17








